Intraductal Papillary Neoplasms of the Bile Duct (IPNB) are uncommon lesions that require a precise, methodical approach to both diagnosis and treatment. For patients, navigating this condition can be challenging due to its scarcity, while for clinicians, it represents an evolving area of biliary pathology.
Recognized as a distinct entity in the World Health Organization (WHO) classification of digestive system tumours, IPNB is a pre-cancerous condition characterized by the growth of papillary masses within the lining of the bile ducts. Because of its high malignant potential, understanding its clinical features and distinct subtypes is essential for achieving an optimal long-term cure.
What is IPNB?
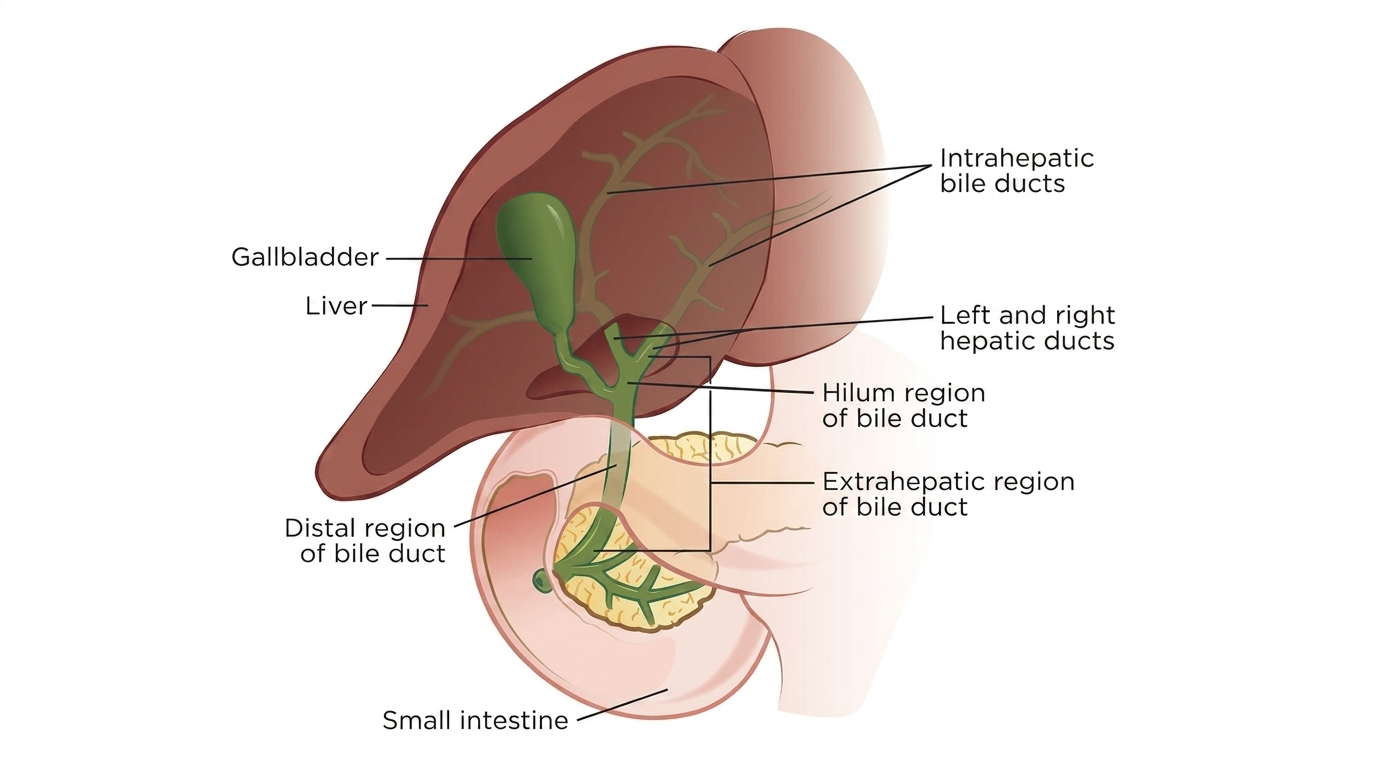
IPNB is considered the biliary counterpart to Intraductal Papillary Mucinous Neoplasms (IPMN) of the pancreas. These tumours develop along the mucosal surface of either the intrahepatic (inside the liver) or extrahepatic (outside the liver) bile ducts.
A defining feature of many IPNB lesions is the hypersecretion of mucin—a thick, gelatinous fluid. As the papillary tumour grows and produces this material, it obstructs the normal flow of bile, creating intermittent biliary hypertension. This leads to a phenomenon known as mucobilia, which causes diffuse or segmental dilation of the biliary tree.
The Diagnostic Challenge
IPNB can be difficult to identify early because its clinical presentation closely mimics much more common, benign biliary conditions, such as gallstones or benign strictures. Patients frequently present with a triad of non-specific symptoms:
- Intermittent right upper quadrant abdominal pain
- Recurrent bouts of cholangitis (bile duct infection) accompanied by fever and chills
- Transient or progressive jaundice (yellowing of the skin and eyes)
Because pieces of the friable papillary tumour or plugs of thick mucin can pass dynamically through the ductal system, symptoms and liver function test results often fluctuate. This variable clinical picture frequently leads to diagnostic delays on standard ultrasound or CT imaging, where the tumour itself may be barely visible beneath the severe ductal dilation.
Advancements in Preoperative Mapping
To overcome these challenges, a multimodality imaging approach is required. Magnetic Resonance Cholangiopancreatography (MRCP) is highly valuable for evaluating the exact geometry of the biliary dilation and identifying intraluminal filling defects.
However, because IPNB has a strong propensity for superficial mucosal spreading along the bile ducts, conventional radiology often underestimates the true extent of the disease.
To achieve an accurate blueprint for surgery, modern digital peroral cholangioscopy (such as SpyGlass technology) has become a vital tool. This allows the specialist to pass a small camera directly into the biliary tree to visually inspect the mucosa, identify the precise borders of the papillary projections, and obtain targeted biopsies.
Classification: Type 1 vs. Type 2
The international consensus subclassifies IPNB into two major clinicopathological types, which dictate both the surgical boundaries and the long-term outlook:
- Type 1 IPNB: Most commonly located within the intrahepatic bile ducts. It features a more regular, well-organized cellular architecture and shares strong molecular characteristics with pancreatic IPMN. Patients with Type 1 lesions generally experience a more indolent disease course and a highly favourable post-operative prognosis.
- Type 2 IPNB: Predominantly found in the extrahepatic biliary system. This variant exhibits an irregular, complex structural architecture, a higher baseline grade of cellular dysplasia, and a significantly more aggressive clinical course.
The Necessity of Radical Surgical Resection
Unlike certain low-risk pancreatic cysts that can be safely monitored through long-term surveillance, IPNB requires proactive, definitive treatment. Surgical resection is the established standard of care.
Clinical registry data indicates that between 40% and 80% of IPNB cases already harbor an associated invasive carcinoma component (invasive cholangiocarcinoma) at the time of operation.
Consequently, the surgical strategy must be meticulously planned by a specialist. Achieving an R0 resection—meaning completely negative surgical margins—is the single most critical factor in preventing local recurrence.
During the operation, the use of intraoperative frozen section analysis is essential to evaluate the cut edges of the bile duct, ensuring no microscopic superficial disease is left behind. Depending on the location and extension of the tumour, achieving clearance may necessitate a formal liver resection (hepatectomy), an extrahepatic bile duct resection with reconstruction, or a pancreaticoduodenectomy (Whipple procedure).
Summary
IPNB sits on a clear continuum between benign ductal obstruction and invasive biliary malignancy. When a patient presents with unexplained bile duct dilation, mucin production, or recurrent cholangitis without a clear history of gallstones, IPNB must be considered in the differential diagnosis. Early recognition, comprehensive preoperative mapping, and complete surgical clearance offer the most reliable path to a permanent cure.