Laparoscopic cholecystectomy (gallbladder removal) is one of the most common operations performed worldwide. Because it is routine, there is a tendency to view it as “simple.” However, as an HPB surgeon, I often remind my trainees and my patients of a crucial fact: while the procedure is standardized, the anatomy is not.
Every human body is unique. Just as our facial features differ, so does the internal “roadmap” of our biliary system. Understanding anatomical variations is the key to performing safe, effective surgery.
The Standard Roadmap vs. Reality
In medical textbooks, the anatomy looks predictable. The gallbladder connects to the main bile duct via a small tube called the cystic duct, and it is fed by a single cystic artery. We often visualize this area as a roadmap where a driveway (cystic duct) connects a house (gallbladder) to the main highway (common bile duct).
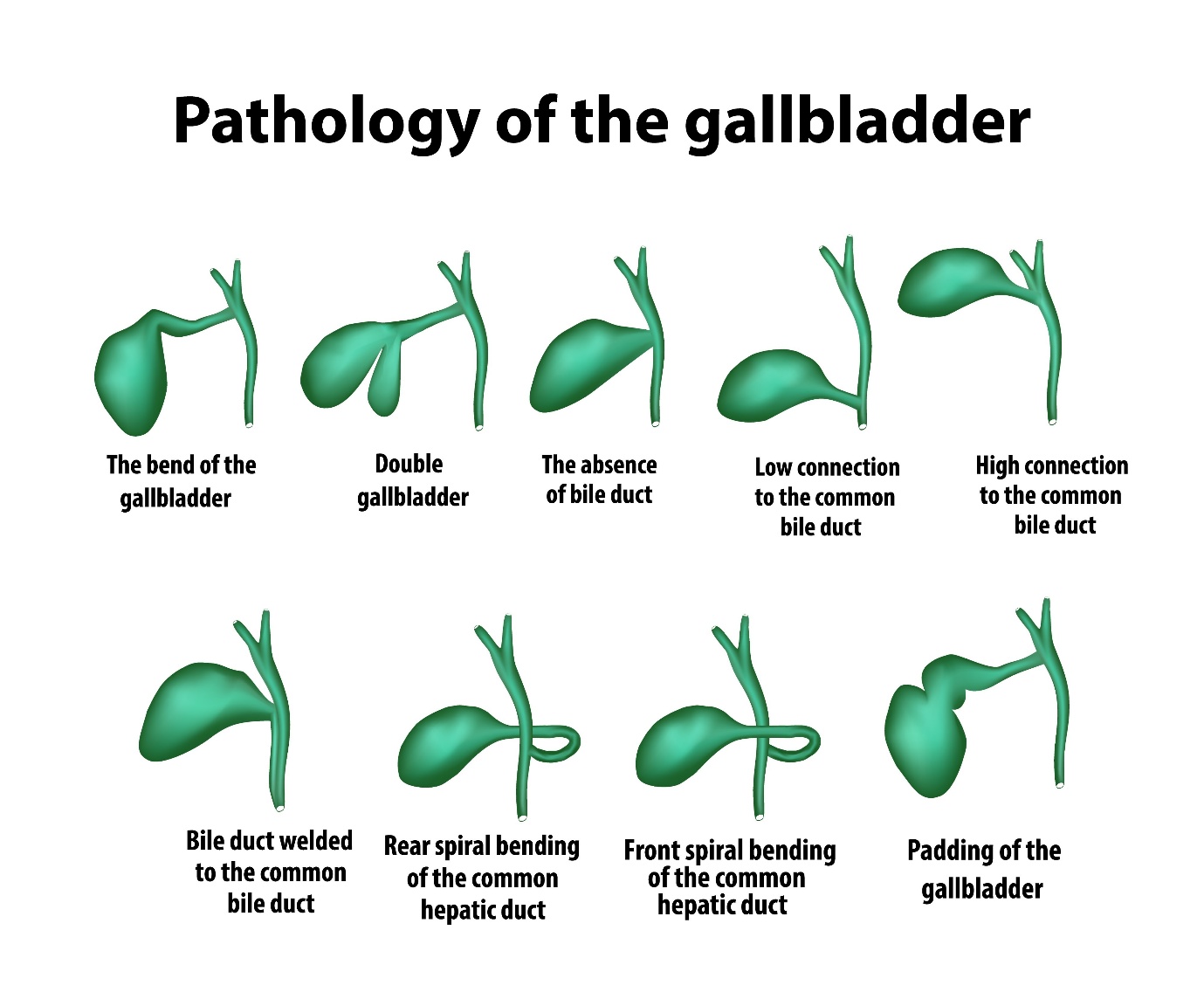
However, in the operating room, reality often deviates from the textbook. Anatomical variations occur in a significant percentage of the population. These are not “defects” or signs of poor health; they are simply normal deviations of human development.
Common Variations We Encounter
The most critical portion of a laparoscopic cholecystectomy involves dissection of the HepatocysticTriangle. For my patients, this is the critical zone where we must separate the gallbladder from its attachments without injuring the main bile duct or blood vessels.
Here are a few variations that require an expert eye:
The Short Cystic Duct: Sometimes, the “driveway” is virtually non-existent, meaning the gallbladder sits directly on the main “highway.” Mistaking the main duct for the cystic duct is a major risk, requiring meticulous dissection.
Moynihan’s Hump (Tortuous Hepatic Artery): In some cases, the right hepatic artery loops dangerously close to the gallbladder, resembling the hump of a caterpillar. If a surgeon assumes the artery is in its “standard” location, this loop can be accidentally injured.
Accessory Ducts (Ducts of Luschka): These are tiny, extra drainage channels that run directly from the liver into the gallbladder bed. If missed, they can cause minor but annoying bile leaks after surgery.
Aberrant right posterior sectoral duct: A duct that drains a significant portion of the liver may travel through the hepatocystic triangle. If it is not identified and inadvertently divided, the repair can require complex reconstruction surgery or liver resection.
The Solution: The Critical View of Safety
How do we ensure safety when the anatomy is unpredictable? We utilize a technique called the Critical View of Safety (CVS).
I do not simply clip structures because they “look” right. Instead, I meticulously clear the fat and fibrous tissue around the gallbladder’s neck. I must clearly see two—and only two—structures entering the gallbladder (the duct and the artery) and separate the lower third of the gallbladder from the liver bed before any clips are applied.
When in Doubt: The Intraoperative Cholangiogram (IOC)
Sometimes, even the Critical View isn’t enough. Inflammation can distort the tissue, or the anatomy may be so unique that it defies standard description. In these moments, we don’t guess; we use technology to “light up” the roadmap. This is called an Intraoperative Cholangiogram (IOC).
Think of the biliary system like a plumbing network hidden behind a wall. We can see the pipes on the outside, but we can’t always see where they flow inside the liver or if there are blockages deep within.
How it works: During the laparoscopy, I insert a tiny catheter into the cystic duct and inject a special radiopaque dye. We then take a live X-ray video.
Why this step is critical:
Definitive Mapping: The dye fills the bile ducts, creating a clear map on the monitor. This proves exactly which duct is which, ensuring we are cutting the cystic duct and not the common bile duct.
Detecting Hidden Stones: Sometimes, a gallstone can escape the gallbladder and get stuck in the main highway (the common bile duct). The IOC reveals these “roadblocks” (seen as dark spots in the dye) so we can address them immediately.
Frequently Asked Questions
Patients often have specific worries when they hear about “anatomical variations.” Here are the answers to the questions I hear most often:
Q: If I have an anatomical variation, does that make my surgery “high risk”?A: Not necessarily. Variations are actually quite common (up to 20-30% of people have some deviation). It only becomes a risk if the surgeon doesn’t recognize it. Once we identify the variation, the surgery proceeds just as safely as a standard case.
Q: Will I know if I had a variation after the surgery?A: I usually mention it in my post-operative notes or tell you briefly after the procedure. However, for you, the recovery process remains exactly the same. Your body functions normally whether your cystic duct was short, long, or spiral.
Q: What happens if you can’t see the anatomy clearly due to inflammation?A: If the “Critical View” cannot be achieved safely, I will never force it. I may perform a “subtotal cholecystectomy” (removing the diseased part of the gallbladder but leaving the tricky bottom part attached to protect the duct), or in rare cases, convert to an open surgery. These are safety decisions, not failures.
Q: Does an Intraoperative Cholangiogram expose me to a lot of radiation?A: No. The amount of radiation from the X-ray used during an IOC is very low—comparable to a standard chest X-ray. The benefit of ensuring your bile ducts are safe far outweighs this minimal exposure.
A Final Note
If you are scheduled for a cholecystectomy, know this: speed is never my goal. Identification is. I approach every surgery expecting variations. This mindset—anticipating the unexpected—is what prevents complications and ensures a routine, safe recovery.